yyzzhh 管理员 昵称:忙! 等级: 叩诊锤主任医师 勋章: 发贴: 4720 贴 总积分: 701 分 第27期 评奖积分: 0 分 注册: 2007-03-30
#1 2008-1-25 14:49:00
典型影像,大家看看
A:平扫MRI T1
B:增强MRI T1
C:质子相
D:T2
查看此帖需要积分0 分
plateauhawk 昵称: 等级: 叩诊锤实习医师 发贴: 19 贴 总积分: 6 分 第27期 评奖积分: 0 分 注册: 2007-10-27
#2 2008-1-25 15:26:00
Re:典型影像,大家看看
什么东东?脑囊虫!!!!!!!
查看此帖需要积分0 分
yyzzhh 管理员 昵称:忙! 等级: 叩诊锤主任医师 勋章: 发贴: 4720 贴 总积分: 701 分 第27期 评奖积分: 0 分 注册: 2007-03-30
#3 2008-1-25 16:02:00
Re:典型影像,大家看看
上面的图片不清楚,发另一个病人的MRI增强片:
本贴已被 作者 于 2008-1-25 16:2:45 编辑过
查看此帖需要积分0 分
小不点120 昵称: 等级: 叩诊锤实习医师 发贴: 8 贴 总积分: 1 分 第27期 评奖积分: 0 分 注册: 2008-01-24
#4 2008-1-25 16:31:00
Re:典型影像,大家看看
脑沟加深,加增.脑白质见星粒改变.应该是"脑囊虫"吧
查看此帖需要积分0 分
xie780804 昵称:青囊行者 等级: 叩诊锤实习医师 发贴: 10 贴 总积分: 3 分 第27期 评奖积分: 0 分 注册: 2008-01-16
#5 2008-1-25 17:12:00
Re:典型影像,大家看看
强烈要求提供病史、查体资料!
查看此帖需要积分0 分
w88w 昵称: 等级: 叩诊锤副主任医师 发贴: 439 贴 总积分: 120 分 第27期 评奖积分: 0 分 注册: 2007-11-13
#6 2008-1-25 21:32:00
Re:典型影像,大家看看
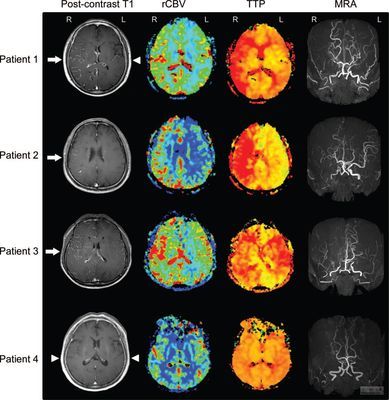
增强扫描可以发现软脑膜增强,提示炎性疾病或者脑膜癌。这些不好解释患者脑室周围缺血改变。
脑膜炎?
血管炎?
脑膜癌?
查看此帖需要积分0 分
yyzzhh 管理员 昵称:忙! 等级: 叩诊锤主任医师 勋章: 发贴: 4720 贴 总积分: 701 分 第27期 评奖积分: 0 分 注册: 2007-03-30
#7 2008-1-26 13:03:00
Re:典型影像,大家看看
患者术中的图片:
本贴已被 作者 于 2008-1-26 13:4:4 编辑过
查看此帖需要积分0 分
chinastroke 名誉版主 昵称:I'm Wall.E 等级: 叩诊锤主治医师 发贴: 1961 贴 总积分: 232 分 第27期 评奖积分: 0 分 注册: 2007-06-30
#8 2008-1-26 13:08:00
Re:典型影像,大家看看
Quote: 以下是引用 yyzzhh 于 2008-1-26 13:03:24 的发言
患者术中的图片:
我明白了,软脑膜强化有一种原因为分布在软脑膜上的血管显著增多,这样造影剂在小血管中出现潴留,因此可看到软脑膜强化的情况。
脑膜癌的软脑膜强化和moyamoya的软脑膜强化机理是不是一样的呢?
这是不是也说明只要存在严重的软脑膜血管增生就会出现软脑膜强化呢?
Sorry!
永远支持论坛!
查看此帖需要积分0 分
zxp2005282 昵称: 等级: 叩诊锤住院医师 发贴: 94 贴 总积分: 30 分 第27期 评奖积分: 0 分 注册: 2007-06-29
#9 2008-1-26 16:15:00
Re:典型影像,大家看看
I got it
"Ivy Sign" in Moyamoya Disease.注:常春藤征(ivy sign)
look!
点击下载
and
点击下载
本贴已被 作者 于 2008-1-26 16:47:16 编辑过
查看此帖需要积分0 分
yyzzhh 管理员 昵称:忙! 等级: 叩诊锤主任医师 勋章: 发贴: 4720 贴 总积分: 701 分 第27期 评奖积分: 0 分 注册: 2007-03-30
#10 2008-1-26 20:02:00
Re:典型影像,大家看看
哈,的确是典型的ivy sign
公布答案:MoyaMoya病
Figure 1. MR images of Patient 1 before the operation. A, precontrast T1-WI (TR, 400 ms; TE, 20 ms; 1 NEX). Several flow-void spots are seen corresponding to some cortical vessels (arrows). B, postcontrast T1-WI with Gd-DTPA (TR, 400 ms; TE, 20 ms; 1 NEX), showing diffuse leptomeningeal enhancement along cortical sulci, like ivy creeping between stones. The flow-voids seen in A remained almost the same (arrows). C, proton density image (TR, 2000 ms; TE, 30 ms; 1 NEX). Multiple flow-voids are seen in basal ganglia. D, T2-WI (TR, 2000 ms; TE, 90 ms; 1 NEX) shows subcortical highintensity lesions.
Figure 2. Carotid angiograms of Patient 1 before the operation. A and B, right carotid angiograms showing narrowing at the terminal portion of the internal carotid artery (arrow), basal moyamoya in evolution (large arrowheads), ethmoidal moyamoya in early stage (small arrowheads), parietal cortical arteries visualized via leptomeningeal anastomosis from posterior cerebral artery (open arrowheads). Cortical branches of the ACA and the MCA are poorly visualized. C and D, left vertebral angiograms showing marked retrograde filling into the territory of ACA and MCA via leptomeningeal anastomosis
Figure 3. Intraoperative view of Patient 1. Markedly profuse pial arterial network diffusely covers the cortex.
Figure 4. MR images of Patient 1 after the operation. A, precontrast T1-WI (TR, 400 ms; TE, 20 ms; 1 NEX) showing subtle increase in the cortical flow-void spots compared with Fig. 1A. B, postcontrast T1-WI with Gd-DTPA (TR, 400 ms; TE, 20 ms; 1 NEX) showing significant reduction in the leptomeningeal enhancement observed in Fig. 1B. C, proton density image (TR, 2000 ms; TE, 30 ms; 1 NEX). Multiple flow-voids in basal ganglia decrease compared with Fig. 1C. D, T2-WI (TR, 2000 ms; TE, 90 ms; 1 NEX) showing decrease in the subcortical high-intensity lesions.
Figure 5. Postoperative angiogram of Patient 1. A and B, right external carotid angiogram. Branches of MCA are opacified via surgical and leptomeningeal anastomosis. C and D, left external carotid angiogram. Similar findings as in A and B.
本贴已被 作者 于 2008-1-26 20:7:2 编辑过